
After years of criticism that the current distribution of primary care funding is not meeting the needs of deprived areas, the government’s 10 Year Health Plan has committed to reviewing how money is distributed. Here, Dr Laura Anselmi presents an updated approach which draws on patient data to more accurately reflect the prevalence of different health needs.
- The current funding model for general practices in England includes a weighted component, based on registered patients’ age and gender, among other factors.
- However, this formula has not been updated since 2004, and was based on data from a small number of practices.
- A new formula uses richer, more recent data, combined with new weighting criteria, to more closely reflect the needs of patients.
General practices in England are funded through a mixed payment system. Around 60% of payments are based on the number of patients registered with a practice, weighted by their needs (weighted capitation). Other payments are based on the services delivered, either by volume, or by quality on a range of indicators, while additional payments support operations, such as for premises or IT.
The weighted capitation component is informed by the Global Sum formula (also known as the Carr-Hill formula), which seeks to predict practices’ workload through measures of population needs. It also adjusts for the costs of providing services in different locations, such as those with high prices, or rural areas. The formula has not been updated since 2004, and there are long-standing concerns that it does not adequately reflect current needs, particularly those of practices in more deprived areas.
The 10 Year Health Plan for England committed to a review of “how health need is reflected in nationally determined contracts”, including Carr-Hill. This review was launched in October 2025 and is currently ongoing.
An updated workload formula accounting for morbidity
A key element of Carr-Hill is the workload weights, estimated using patient data from under 5% of general practices in 2004. Workload was defined as appointment time with patients of different general practice professionals. It considered only age, gender, new registration, and whether the appointment took place at home or in a nursing home. A separate area-level adjustment was applied based on rates of long-standing illness and under-65 mortality in the local areas. Despite attempts to revise it and more recent formulae used for allocations, the formula used for practice payments has not been updated for over 20 years.
Our research at The University of Manchester proposes an updated, refined approach to calculate workload weights using more recent, nationally-representative patient-level data from electronic health records, which now cover over 20% of patients and general practices in England. Workload weights were generated based on patients’ age; gender; new registration; ethnicity; deprivation; and long-term conditions (LTCs), such as diabetes, asthma, or arthritis.
The use of richer data from electronic records allowed us to separate variations attributable to patients’ and practices’ characteristics, and to estimate workload driven by patients’ need characteristics. One advantage is that the updated measure of workload would be needs-based and not reflect differences in practice capacity and productivity.
We found estimated workload increases with age, deprivation, and for patients with LTCs. The inclusion of LTCs increases workload differentiation between patients, adding weight to younger patients in less deprived areas and older patients in more deprived areas. It also better reflects, on average, the higher needs of practices serving patients in more deprived areas.
Comparing updated to Carr-Hill workload weights
We obtained updated needs-based estimates of workload for each general practice in England, using weights from the updated formula and publicly available data on the number and characteristics of patients in each practice in 2024. For each practice we acquired a measure of “weighted-patient” – derived from the latest practice data and the updated weights – summarising the needs-based workload per average patient relative to the national average. The average payment per-patient per-year, excluding the cost-adjustment for differential input prices across different areas (also called Market Forces Factor, MFF), was £92.66, varying from £86.72 in the least deprived decile to £99.91 in the most deprived.
Weighting payments to account for different health needs leads to a slight reduction in these figures, ranging from £89.69 in the least deprived decile, to £96.40 in the most deprived. This suggests that current payments per-patient are relatively higher for practices serving patients in more deprived areas, even after adjusting for needs reflected in workload.
Carr-Hill weighted-patients were on average higher than the updated ones for practices serving patients in more deprived areas. This was likely driven by the separate area-level adjustments for long-standing illness and under-65 mortality. We attempted to isolate the workload component of Carr-Hill by removing the MFF component, though we could not remove the cost adjustment for rurality. The Carr-Hill weight on practices serving populations in more deprived areas was even higher after removing the MFF.
Comparisons of average weighted-patient by practice deprivation decile
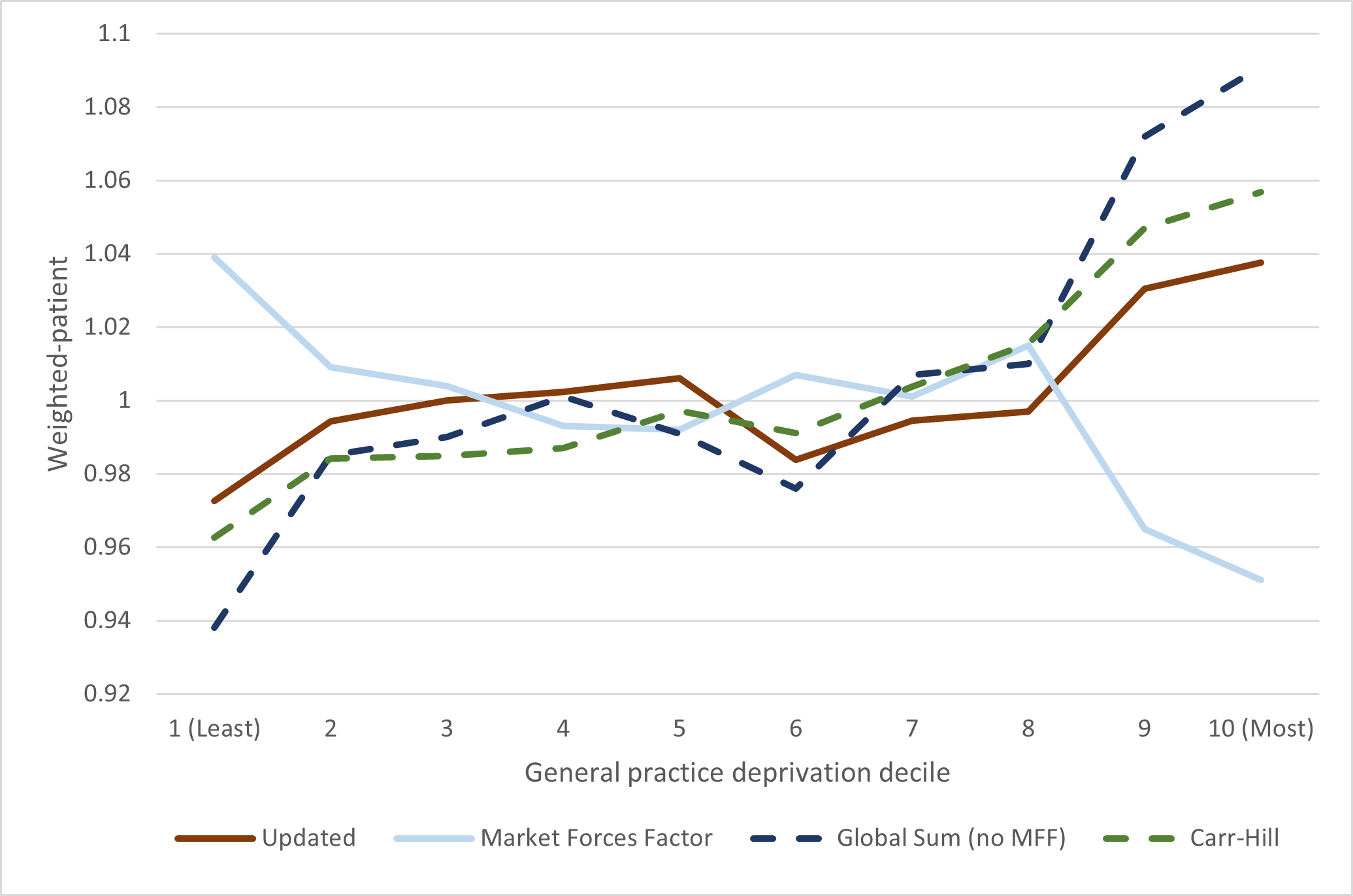
Adapted from paper.
Aligning payments to updated workload weights
It is possible to uplift payments per weighted-patient to the level of better funded practices to rebalance the distribution without reducing payments for any of the practices. This would require additional funding. For example, it would require approximately £10 per-patient – or £678 million in total – to uplift payments to the level of the 10% best funded practices in 2023/24 (an increase of 11% in the total capitation payments in that year).
Average payment per-patient by practice deprivation decile under different uplift scenarios (2023/24)
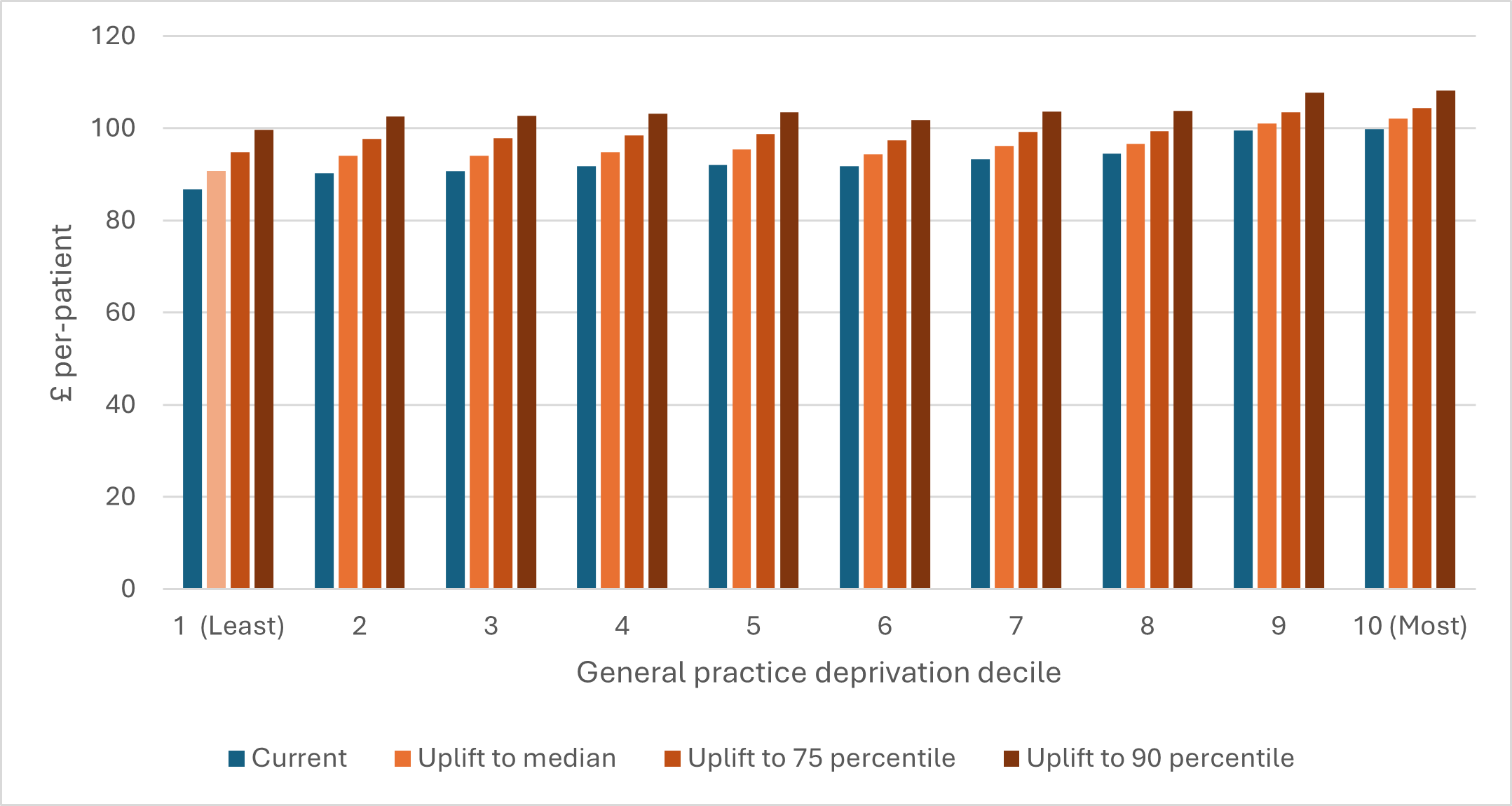
Adapted from paper.
Policy implications
The core principle of needs-based capitation is the distribution of payments in proportion to patient need. The Carr-Hill formula is outdated and does not reflect needs accurately.
The workload weights of the general practice formula should be replaced with a version which can be routinely updated to reflect changing needs and accounts for a richer set of patient characteristics, ensuring that practices are better resourced for the populations they serve. Our updated estimates provide a more precise and differentiated measure, reflecting higher workload for practices serving patients with higher levels of morbidity and in more deprived areas. National primary care electronic records should be made accessible and used to continue routinely improving workload estimates.
Remaining concerns about under-funding of practices in deprived areas should be considered separately. For example, they could be addressed by adjustments to other elements of the formula, such as a re-evaluation of the MFF adjustment or separate adjustments to account for specific additional needs associated with deprivation. Moreover, if the objective was to increase resources for practices serving populations in more deprived areas, the distribution of the remaining non-capitation payments could also be re-considered. It is likely that any changes to the formula will require additional funding, because simply redistributing existing resources may lead to a reduction in care in some areas, and can be practically unfeasible.
A modern health system depends on funding models that can keep pace with the changing needs of its population. Our evidence shows Carr‑Hill no longer reflects the realities of morbidity, deprivation, and patient complexity across general practices. Using richer, nationally representative electronic health records offers a more accurate and equitable basis for allocating resources, particularly for practices serving communities with higher levels of long‑term conditions and deprivation. Yet an improved formula cannot, on its own, resolve persistent under‑funding in deprived areas; this will require parallel reconsideration of other components, as well as a willingness to invest additional resources where they are most needed. As the government’s review progresses, the adoption of an updated, data‑driven approach to workload estimation offers a critical opportunity: to ensure primary care funding aligns more closely with patient need, and ultimately to strengthen the fairness, sustainability, and effectiveness of general practice across England.
Statement of conflict of interest
This project was supported by the Health Foundation (FR-0006010). This project concluded prior to the launch of the government review into the GP funding formula in October 2025.
The views expressed are those of the authors and not necessarily the funders of the original or subsequent research.
The co-authors of this research, who also contributed to this article, are: Dr Shaolin Wang, Dr Yiu-Shing Lau, Dr Michael Anderson, Professor Evan Kontopantelis, and Professor Matt Sutton.